When planning an implant restoration, one of the earliest decisions you face is retrieval: screw-retained or cement-retained. Both options are clinically proven. Both can deliver excellent outcomes. But they are not interchangeable — and the choice you make affects everything downstream, from the lab work we fabricate to the long-term maintenance your patient experiences.
This guide covers the clinical rationale behind each option, the indications that favor one over the other, and what BioDent’s team needs from you to fabricate either correctly.
What Is a Screw-Retained Implant Crown?
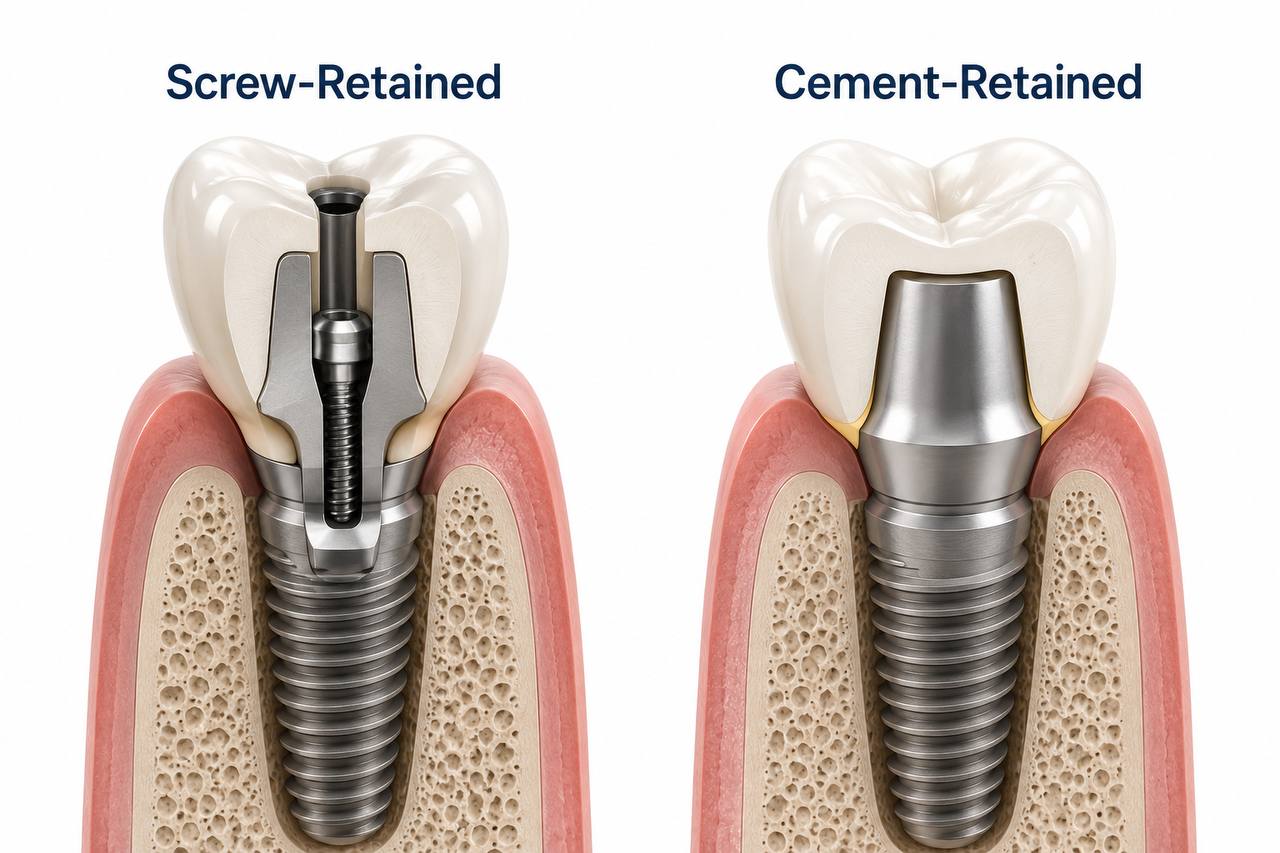
A screw-retained crown attaches directly to the implant or abutment using a titanium screw that passes through the crown itself. The access channel — the small opening on the occlusal or lingual surface — is filled with composite after seating.
The defining characteristic is retrievability. If you need to access the implant, remove the prosthesis, or modify the restoration, you unscrew it. No crown removal, no risk of damaging surrounding tissue, no cement excavation.
At BioDent, screw-retained restorations are fabricated as a single integrated unit — the crown and the interface are designed together in CAD, which allows us to control the emergence profile, margin placement, and access channel angle from the start of the case.
What Is a Cement-Retained Implant Crown?
A cement-retained crown sits on a separate abutment and is secured with dental cement — either temporary or permanent, depending on your intended retention strategy. From the outside, it looks identical to a natural crown preparation.
The prosthetic workflow is closer to conventional crown-and-bridge, which is why many dentists are more comfortable with it early in their implant experience. The crown has no access hole, which gives you full freedom in occlusal design and esthetics.
The tradeoff is retrievability. If anything needs to be addressed at the implant level, the crown must come off — and if permanent cement was used, that often means destroying it.
What Is a Screw-Retained Implant Crown?
A screw-retained crown attaches directly to the implant or abutment using a titanium screw that passes through the crown itself. The access channel — the small opening on the occlusal or lingual surface — is filled with composite after seating.
The defining characteristic is retrievability. If you need to access the implant, remove the prosthesis, or modify the restoration, you unscrew it. No crown removal, no risk of damaging surrounding tissue, no cement excavation.
At BioDent, screw-retained restorations are fabricated as a single integrated unit — the crown and the interface are designed together in CAD, which allows us to control the emergence profile, margin placement, and access channel angle from the start of the case.

When to Choose Screw-Retained
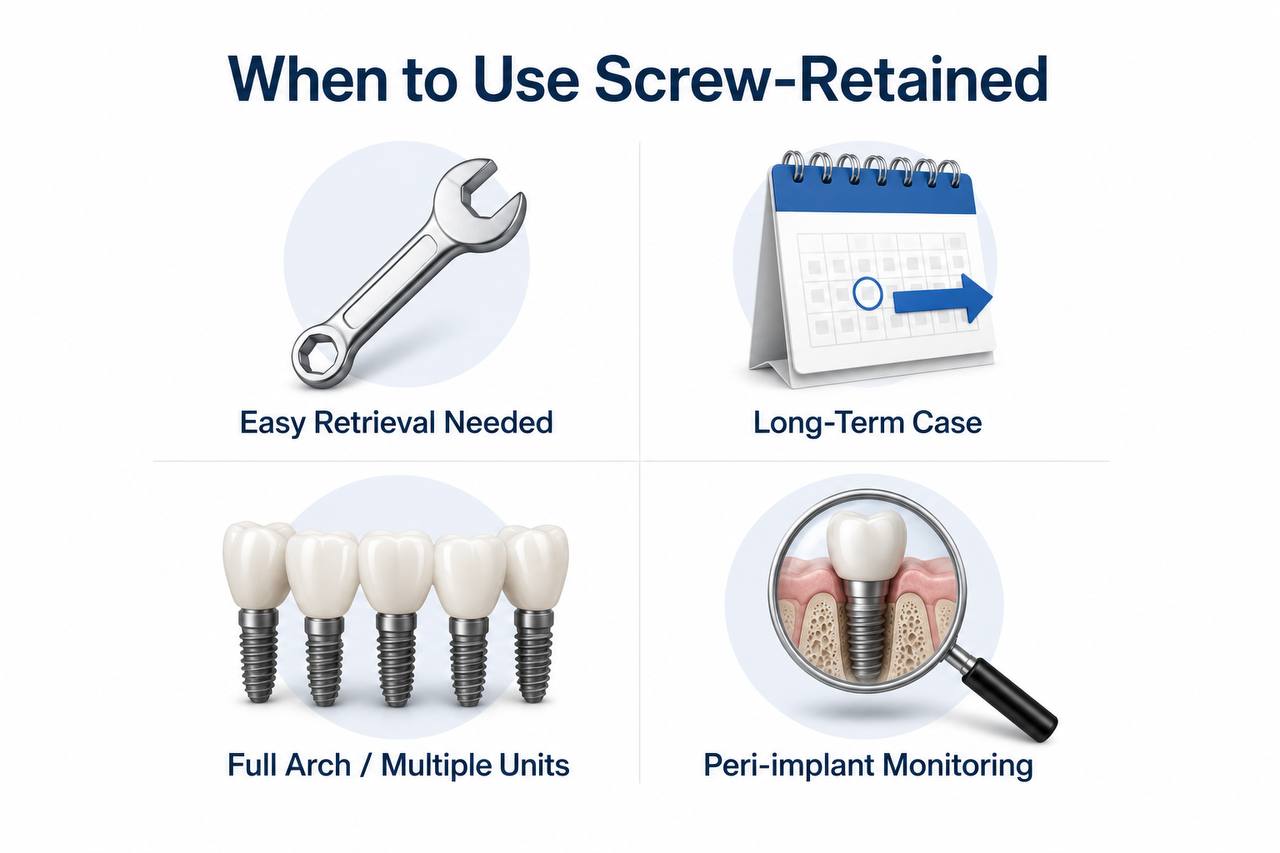
Retrievability is the primary clinical driver. If you anticipate needing access to the implant — whether for peri-implant maintenance, abutment adjustment, or prosthetic modification — screw-retained is the safer long-term choice.
Screw-retained restorations are particularly well suited when:
The implant is in the posterior region and occlusal esthetics are not the primary concern. The access channel on a molar or premolar is easy to position and restore without affecting the final outcome.
The patient has a history of peri-implant complications or requires more frequent monitoring. Being able to remove the prosthesis without risk of fracture or tissue trauma simplifies long-term management significantly.
You are treating a younger patient where the restoration may need to be modified or replaced over decades. Non-destructive retrievability becomes more valuable the longer the prosthesis is expected to function.
The case involves multiple implants or a full-arch prosthesis. In complex cases, the ability to remove individual units or the full bridge for maintenance, implant-level assessment, or repair is a major clinical advantage.
When to Choose Cement-Retained
Cement-retained restorations have genuine clinical advantages in specific scenarios, and dismissing them entirely is not supported by the evidence.
Choose cement-retained when:
The implant angulation is not ideal and a screw access channel would emerge in an esthetically or functionally compromised position. A well-placed custom abutment can correct for off-axis angulation in ways that allow a cement-retained crown to deliver a better final result.
The case is in a high-esthetic zone — upper anterior, for example — where full occlusal design freedom is essential and the absence of an access channel significantly improves the outcome. With careful cement management and the use of retrievable cement, the retrievability concern can be mitigated.
The patient’s bite or parafunction makes access channel sealing unreliable. Some high-force occlusal environments make composite-sealed access channels more prone to long-term failure.
The restorative workflow needs to mirror conventional crown-and-bridge closely — for example, when the dentist is transitioning into implant restorations and a familiar preparation, impression, and delivery process reduces the margin for error.
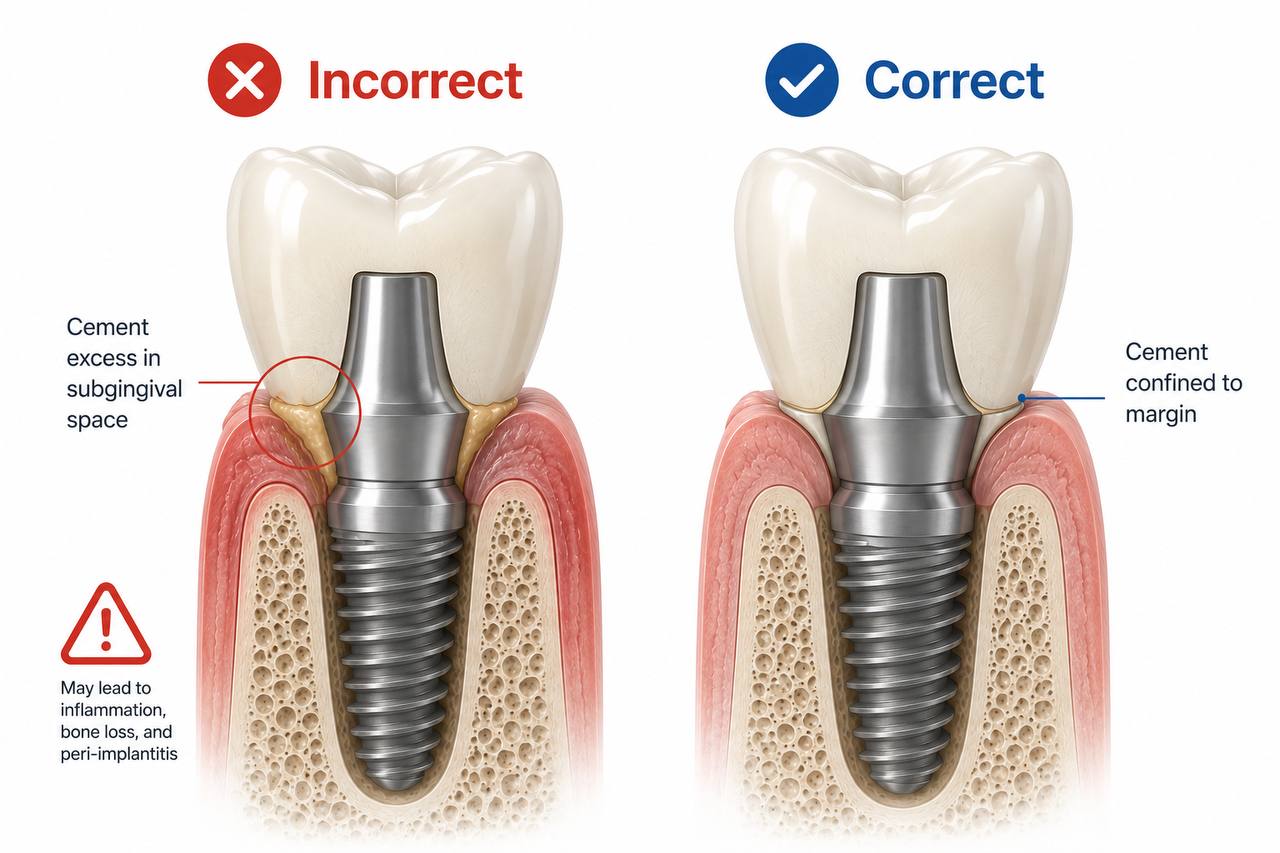
The Cement Excess Problem — and How to Manage It
The most significant risk with cement-retained implant crowns is subgingival cement excess. Residual cement in the peri-implant sulcus is a documented cause of peri-implantitis and can lead to bone loss, tissue inflammation, and eventual implant failure.
This risk is not inherent to cement-retained crowns — it is a function of how they are placed. Several strategies reduce it substantially:
Use a retrievable cement rather than permanent bonding cement. This gives you the option to remove the crown non-destructively if needed.
Have the crown fabricated with a margin positioned at or slightly above the gingival margin where possible, particularly in cases where subgingival depth makes visual access difficult.
Apply cement to the crown interior, seat firmly, and remove excess before it sets — using a technique that directs excess coronally rather than apically.
At BioDent, when fabricating cement-retained cases, we can adjust the internal crown geometry and margin profile to facilitate easier cement management during delivery.
What BioDent Needs to Fabricate Each Option
The information you send with your case directly affects what we can fabricate — and how precisely we can do it.
For screw-retained restorations:
Send the implant manufacturer, system name, implant diameter, and platform connection. A scan of the implant position using a scan body is required for digital cases. Include the opposing arch scan and bite registration. If you have a specific access channel angulation preference, note it.
Without accurate implant position data, we cannot design the emergence profile or screw channel angle correctly.
For cement-retained restorations:
Send the abutment type and dimensions if using a stock abutment, or the implant data if we are fabricating a custom abutment. Include soft tissue scan data where possible — it allows us to design the emergence profile in relation to the actual gingival contour, not a generic estimate. Note your intended cement and margin depth preference so we can design accordingly.
In both cases, the more information you provide upfront, the fewer remakes and adjustments at delivery.
The Most Common Mistakes — and How to Avoid Them
Choosing based on habit rather than indication. The most common error is defaulting to cement-retained because it feels familiar, or to screw-retained because it is currently considered the more modern option. The choice should follow the clinical situation, not the trend.
Incorrect implant position data. A screw-retained crown designed without accurate implant scan data will have a misaligned access channel, poor emergence profile, and likely require adjustment at seating. This is a lab workflow problem that originates at impression or scan stage.
Ignoring long-term retrieval. A cement-retained crown placed with permanent cement in a patient who will need ongoing implant monitoring is a problem deferred, not a problem avoided.
Under-specifying the case. Sending an implant case with just “Nobel, 4mm” is not enough for us to fabricate accurately. System name, platform, diameter, and connection type all matter.

Frequently Asked Questions
Is screw-retained always better than cement-retained?
No. Both have clear indications and both deliver excellent long-term outcomes when used correctly. Screw-retained offers retrievability advantages; cement-retained offers esthetic and angulation flexibility. The right choice depends on the clinical case.
Can BioDent fabricate both types?
Yes. BioDent fabricates both screw-retained and cement-retained implant crowns across all materials — zirconia, e.max, PFM, and full-cast gold. We work with all major implant systems including Nobel Biocare, Straumann, Zimmer Biomet, BioHorizons, and Implant Direct.
What if my implant angulation makes screw access difficult?
We can design angled screw channel solutions for implants up to approximately 25–30 degrees off-axis. For cases beyond that range, a custom abutment with cement-retained crown is usually the more predictable approach.
How long does fabrication take?
Standard turnaround for single-unit implant crowns is 7–10 business days from receipt of the impression or scan. Rush options are available.
Ready to Send Your Implant Case?
BioDent Laboratory is based in Matawan, New Jersey, and serves dental practices across the United States. Whether your case calls for screw-retained precision or cement-retained esthetic flexibility, our team works directly with your case file to deliver a restoration that fits, functions, and lasts.
